Seriously psychotic Ross is likely to die on the streets in the near future – but only because he is intelligent and eloquent. The mental health services say they cannot act despite concluding that he is a serious danger both to himself and to others, which are the key requirements to trigger action under the Mental Health Act.
The question is: why do they say they cannot act?
Years ago, the psychiatrist at Ross’ first psychotic episode assessment said to me: “Ross is very psychotic. Get him help as soon as possible, but I am not going to section him as he is articulate… If he were less intelligent, I would section.” As a direct consequence of this lack of action, the highly vulnerable Ross ended up destitute in New York where he was seriously sexually assaulted, adding PTSD and paranoia to his psychosis. The system let him down and is still letting him down. It must change.
Danger prevention system failure
The example of Ross is an all too familiar problem in the way that the box checking necessary before you can treat someone against their will under the Mental Health Act is interpreted. To take away the freedom of a person is a very serious act. However, if the person in question is highly intelligent, articulate and can “present well” for a short period during an assessment, they are unlikely to get the help they need, even if it has been proved that they are a danger to themselves and to others.
So, the danger to themselves and to others continues, perhaps until someone is seriously injured or dies.
In a Court of Law, Ross being sectioned would be an open-and-shut case. There is a mass of video, photographic, written and verbal evidence from Ross himself, from family and friends, police officers, mental health professionals, charity workers and members of the public. This proves he is the danger to himself and to others required to detain him under the Mental Health Act.
In the court of the assessing consultant, however, things are different.
Mental health consultants are supposed to combine their impressions of the person in front of them with a review of the previous history and evidence. In most cases, these two elements will be aligned so the decision is simple. In the case of someone like Ross there is a conflict. He is well spoken, charming, incredibly intelligent, a hypnotherapist, actor, improv comedian and writer. He is also in survival mode as he doesn’t believe he is ill, his delusions are his reality, he is the Buddha so the prospect of treatment is terrifying.
He is gaslighting for his life.
He has so far successfully gaslit around 9 very experienced consultants with only one failure, a 90% success rate. That single failure saved his life.
Given the pressures they are under, it seems to be far easier for the assessing professionals to allow themselves to be persuaded by his honeyed words and promises rather than the objective evidence. Words that he has carefully crafted to fit the system, to align with the simple, low cost, non-sectioning “I promise to take my medicine” solution. Pursuing the evidence would lead to a far more difficult, messy, and apparently costly, path.
Only apparently costly – financially. Over the last 2 years, failure to section Ross has conservatively cost the mental health services at least 100 man days, the police at least 40 man days plus many, many days of NHS and ambulance service time. The emotional and psychological harms to his ex-girlfriend and family have been extreme.
Déjà vu
My months of effort paid off. Ross was hospitalised for assessment. I spent 2.5 hours with 3 senior consultants, trying to convince them to keep Ross in a secure facility, that his promises to accept treatment voluntarily were lies. Sadly, and I quote:-
“We know what we are doing. As Ross presents well, I am planning to release him – but I will let the family know if I consider there is a risk to them when I do.” Consultant, Prospect Park Mental Hospital, Reading.
Let that sink in.
The expert stated that he was planning to release Ross, even if he considered that the release would be a risk to the family, but would contact the family to tell them they were at risk…
Ross went AWOL 12 hours later. There was no risk warning. His mother was terrified her own son might assault her again.
Days later, as a direct consequence of the lack of action, his paranoia led him to throw his girlfriend’s possessions off a cliff and then assault her at the very edge. She was terrified for her life. At the command of his delusional voices, he then successfully closed the M4, had multiple arrests for criminal damage, assaulted his mother and ex-girlfriend, captured pets and was hospitalised with severe head injuries when he encountered local drug dealers who had broken into his temporary accommodation.
Déjà vu again
Another hospital assessment after yet another arrest. The same pattern is repeated. I send the consultant the dossier and try to persuade her that Ross is lying exactly as before. But Ross “presents well”, so the consultant decides that to be much more important than the evidence and the history that is repeating itself. He goes AWOL and she retrospectively discharges him, saying that there was nothing she could do. As a direct consequence of the lack of action, days later Ross was arrested at Waterloo for scaring the passengers and has returned to the streets with rapidly deteriorating health. It is winter.
The evidence that Ross is a danger both to himself and to others
The mental health services have a very full dossier on Ross. He has been arrested multiple, multiple times (drunk and disorderly, assaulting and being assaulted etc), his ex-girlfriend has provided a statement to the police detailing his psychotic coercive and controlling behaviour. All the services (mental health, housing, police) have said that he is seriously mentally ill and a danger to himself and to others.
Ross self-medicates with weed, alcohol and tranquilisers he finds in bins. He doesn’t understand what is happening to him and why. His feelings of paranoia and delusions are completely real. He believes that the sources of his feelings and delusional thoughts are external, other people, not his own mind.
Why the failure to act under the Mental Health Act?
If it was a court case and not a mental health case?
Consider: Ross is in the dock for crimes. Both the prosecution and defence agree that the evidence is incontrovertible. Ross makes a statement to the judge that he disagrees. He is articulate and speaks well. The judge decrees that, as Ross has presented well over the few days of the trial and as he has told the court that he is innocent and will behave well in the future, he is free to go.
How would that judgement be viewed?
That is just the judgement that is being made by the hospital consultants.
If it was not a mental health illness?
Image a cab driver with epilepsy. They are allowed to drive as the medication they are on has stopped the seizures for several years. He or she stops taking the medication. They have a seizure while driving and have a serious accident, closing the M4 and they, their passenger and a couple of bystanders are injured. The driver is rushed to hospital for treatment of the injuries and a blood test that shows the seizure was caused by epilepsy.
They are in hospital for a week, but don’t have another seizure during that time. The driver says they are ok – they don’t want to lose the cab driving job. The hospital consultant recommends that they can be discharged and signs the paperwork to say they can resume driving because they have been seizure-free during the week in hospital and the driver has said they feel fine.
How would the GMC feel about that decision? What would a court say about that decision when the driver has another accident and people are injured or die?
How would you feel about that decision?
This is exactly the way that the mental health hospital consultants have behaved towards Ross several times. As a result he has been sexually assaulted and seriously injured multiple times, injured others and very nearly caused serious accidents… How can this lack of action be justified?
Are these the reasons why?
In order to section someone against their will, it has to be established that they are a danger to themselves or to others and that they lack the mental capacity to realise that for themselves. Re Ross, the evidence that this is the case is inconvertible.
One
If they feel they have been wrongly detained, the person has the right to an independent 3 person tribunal within 2 weeks. The tribunal will decide if the section is valid or whether the person should be discharged.
My very strong impression (from references to the tribunal by consultants), is that this puts considerable pressure on the consultant because Ross can be so very, very articulate and plausible. They feel the need to second guess the potential tribunal outcome and are concerned that the section might be overturned.
Which would be awkward.
Two
Almost every consultant with whom I have spoken has given much, much more weight to “the way the person in front of them presents” than to the objective evidence and to the concerns of friends and family. This may be reasonable in most cases, but for exceptionally intelligent and articulate outliers like Ross, this does not work.
There have to be serious safeguards in place to ensure that sectioning cannot be abused, “the evil relative putting granny” in the asylum meme or “I have made a rational decision to chose this unusual lifestyle” cases. Those safeguards are not supposed to prevent the proper sectioning of someone who desperately needs help. For people like Ross, the way that the consultants have interpreted the safeguards can doom them to a terrible life and an early death…
“Safeguarding.” Really?
Three
Resources. That’s it. Just “resources”. There is massive pressure on the mental health services as they have not been given the resources they need concomitant with the damage such illnesses cause. Even on a strict financial basis where mammon rules, “Return on Investment”, mental health problems proportionately cost the UK massively more than the share of the budget accorded the services.
Given the pressure, One and Two come into play, even if subconsciously.
And finally
I have had considerable support from local mental health staff, up to the point when Ross has been taken to hospital. At that point, there have been 2 recent identical failures in the interpretation of the Mental Health Act, ignoring objective evidence and the opinions of family, friends and local mental health professionals in favour of the lies from my son.
I have to try everything and anything I can think of, so I write this and will continue to try to get him sectioned. I have to continue to rage against the dying of my son.
I grieve – and hope that, somehow, at some point, from someone, he will get the help he needs before he, or someone else, is badly injured or dies.
I cannot let him go, and yet I feel he is leaving, that the son I know and love is fading like a dissipating Cheshire Cat, leaving nothing behind but the faintest echo of who he was…
A Father Dreams his Distant Son
Flailing feelings, flailing, blind
He goes away in thought and deed
Lashed by whips that flay his mind
Grasping nets that turn to mist
Grasps and grasps but falls apart
A part of him a part of me
His beat beat beating in my heart
Exhaustion feeds a form of sleep
As father dreams his distant son
Strains to hold a fading ghost
Of the one, the son who’s gone
Drown breaths open floating eyes
Oppressed by deepest, darkest night
I cannot have these feelings yet
With darkness brailling his mind’s sight
I must act with careful calm
As dying thoughts breed deadly schemes
I dredge the words to ward his death
But deep inside, a father screams
Writhing on his spit of love
Impaled again, and torn and torn
Blame barbed spear is pressed so deep
A primal pain that can’t be borne
Then, past a headland, a mirrored loch
Over deathly deeps where lives are lost
Float songs to tempt the tears of hope
I’ll will him well at any cost…
 Burns night meal with friends, 2019. Ross burns bright, the life and soul. 6 weeks later, we use the anniversary of my dad’s death as an excuse to visit the crematorium together, followed by pub lunch. He is – on edge. After food he becomes vocally aggressive, shouting. I have to leave. That evening he emails. He simultaneously never had a mental health problem (my having him sectioned was abuse) and all his mental health problems were caused by me. Schrödinger’s psychosis.
Burns night meal with friends, 2019. Ross burns bright, the life and soul. 6 weeks later, we use the anniversary of my dad’s death as an excuse to visit the crematorium together, followed by pub lunch. He is – on edge. After food he becomes vocally aggressive, shouting. I have to leave. That evening he emails. He simultaneously never had a mental health problem (my having him sectioned was abuse) and all his mental health problems were caused by me. Schrödinger’s psychosis. I spend 2 months putting intense pressure on the local mental health services and finally succeed in persuading them to act. They call to say they will turn up with the team to assess him – on the morning after he burnt down the shed (in which he had been semi-living) in the night and disappeared to, as we later discovered, Bournemouth. I contact the Bournemouth mental health services (local services doing chocolate teapot impressions) and, eventually, he is picked up by the police and taken to Prospect Park hospital in Reading for assessment. Relief is too mild a word. BUT. Fleeting. I’m told that he’s a “trustee”, allowed to come and go as he has promised to be treated in the community. I’m told he will shortly be released into that imaginary community…
I spend 2 months putting intense pressure on the local mental health services and finally succeed in persuading them to act. They call to say they will turn up with the team to assess him – on the morning after he burnt down the shed (in which he had been semi-living) in the night and disappeared to, as we later discovered, Bournemouth. I contact the Bournemouth mental health services (local services doing chocolate teapot impressions) and, eventually, he is picked up by the police and taken to Prospect Park hospital in Reading for assessment. Relief is too mild a word. BUT. Fleeting. I’m told that he’s a “trustee”, allowed to come and go as he has promised to be treated in the community. I’m told he will shortly be released into that imaginary community…
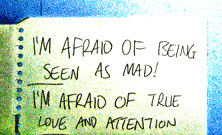 Killed his guitar in the woods on new years night, videoed himself painting his room red and dark green, and put up signs like these everywhere.
Killed his guitar in the woods on new years night, videoed himself painting his room red and dark green, and put up signs like these everywhere. “Yet to be named” was the last thing Ross achieved before crashing. Re-released as with new band as “Consumed in self”.
“Yet to be named” was the last thing Ross achieved before crashing. Re-released as with new band as “Consumed in self”. Smoked dope for a while, but then tried to give up following some scary symptoms. Wrote “Blame Marijuana”, prescient, but sadly too late…
Smoked dope for a while, but then tried to give up following some scary symptoms. Wrote “Blame Marijuana”, prescient, but sadly too late… While I was comatosed
While I was comatosed Get him a doctor
Get him a doctor Let me be nothing
Let me be nothing Going Home
Going Home Song of Sickness
Song of Sickness Chaos
Chaos Hugging Barbed Wire
Hugging Barbed Wire  then where will you go..
then where will you go.. Melancholy
Melancholy  Don’t Fade
Don’t Fade